
Managing chronic hepatitis B.
Chronic hepatitis B (CHB) is a dynamic disease. Ongoing and consistent monitoring is an essential component of CHB management. It is also critical to remain vigilant about regular screening for liver damage and liver cancer, and to routinely monitor patients on CHB treatment for possible nonadherence or the development of resistance.1
Poor monitoring of CHB patients makes determining treatment eligibility more difficult, while suboptimal surveillance predisposes CHB patients to the risks of disease progression, including HCC and its sequelae.2-4
Adherence to CHB treatment and regular follow-up visits are essential for optimal patient health.
People with CHB have a significantly higher prevalence—and risk—of renal disease, and a higher prevalence of cardiovascular, bone, and metabolic diseases than those without CHB.5-7

Lifelong monitoring for CHB patients
Many people with CHB receive suboptimal care and are not adequately monitored for ALT and HBV DNA, leaving them at risk for cirrhosis and HCC.2,3
Every 3-12 monthsb
AASLD 2018 guidance recommends blood tests to monitor HBeAg, HBV DNA, and ALT levels1
| HBeAg | HBV DNA (IU/mL) | ALT | Recommended Follow-up | |
|---|---|---|---|---|
| >20,000 | ≥2xULN or significant histologic diseasec | Treat patients (immune-active CHB) | ||
| >2,000 | ||||
| Detectable | Cirrhosis, regardless of ALT | Treat patients | ||
| ≤20,000 | <2xULN | Consider treatment based on:
| ||
| ≤2,000 | ||||
cLiver biopsy/non-invasive testing showing moderate-to-severe necroinflammatory activity on histology and/or significant fibrosis.
dSerologic and virologic benefits of pegylated interferon occur after treatment discontinuation (delayed). Prior exposure to nucleos(t)ide analogs is a risk for drug resistance.
ePresence of extrahepatic manifestations is an indication for treatment, independent of liver disease severity.
fThis was a retrospective analysis of 1329 CHB patients from the San Francisco Bay Area (January 1996-July 2013).3

Every 6 months
AASLD and AATA recommend ultrasound ± AFP for HCC surveillance with at-risk patients1
AASLD1 | |
|---|---|
Tests | At-risk populations |
|
|
AATA8 | |
|---|---|
Tests | At-risk populations (Asian Americans)g |
|
|
AASLD1 | Tests |
|
|---|---|---|
At-risk populations |
|
AATA8 | Tests |
|
|---|---|---|
At-risk populations (Asian Americans)g |
|
hAFP and CT scan or MRI at 3 months for people with elevated AFP or undergoing HCC treatment.
With routine surveillance:



Support patients’ adherence to CHB treatment
Compared with clinical trials, treatment adherence may be lower in clinical practice. Patients may be less motivated, less frequently monitored, and often have to pay a part of their medication costs.10
Discussing treatment adherence with your CHB patientsEngage in an open dialogue with your patients and listen carefully to their concerns. Encouraging your patients to express what is on their minds may help them become more involved in and committed to their chronic hepatitis B treatment plan.
Advise patients to check with you before taking any new medications, over-the-counter medicines, or herbal supplements, and to let you know if they experience any side effects.11
Urge your patients to take their chronic hepatitis B medicine exactly as prescribed. Explain to your patients that they should not stop taking their chronic hepatitis B medicine without first discussing it with you.11
Suggest medication reminder tools, such as a cell phone app, an alarm clock, or a 7-day pill box, for those patients who are prescribed oral antivirals and need help remembering to take them.
Encourage lifestyle changes for liver health, such as avoiding alcohol and smoking and eating a healthy diet low in saturated fats, with plenty of fruits and vegetables.12
Consider the impact of comorbidities on CHB patients
Due to the associations between CHB infection and comorbidities such as kidney- and bone-related conditions, careful evaluation and consideration are needed when managing CHB patients.1
In the US, the CHB patient population is growing older and has more comorbidities as they age.7,13
Two studies reported the prevalence of comorbidities in US CHB patients significantly increased over time (2000-2005 vs 2011-20157and 2006 vs 201513), including:





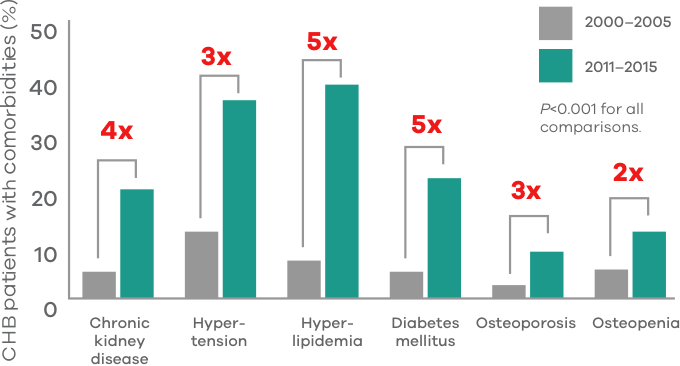
iA retrospective, observational study of 2734 CHB patients across 3 time periods (2000–2005; 2006–2010; 2011–2015) at a university medical center and primary care clinics in the San Francisco Bay Area.7
Renal function typically decreases with age and renal impairment (eg, CKD, ESRD) is observed more frequently in CHB patients than in uninfected people.5,6,14
Cumulative incidence of CKD and ESRD in untreated, Taiwanese CHB cohort5,6


Two nationwide, Taiwanese cohort studies using the Taiwan National Health Insurance Research Database, to evaluate the association of HBV with CKD (inclusive of stages 1 to 5) (1998-2010; N=17,796) or ESRD (1999-2010; N=17,758).5,6

Bone density may decrease with age, and osteoporosis and bone fracture are observed more frequently in CHB patients than in uninfected people.13,15
Prevalence of osteopenia and osteoporosis in a Chinese cohort15,k


kA study conducted in China (2014-2015) of 148 CHB patients vs age- and gender-matched healthy controls, to investigate the prevalence of osteoporosis in CHB patients.16

